【概 要】

・「呼吸器系の機能の中心であり、肺の実質として最も重要な部分」(船戸和也のHP)
・「肺胞同士は非常に接近しており隣り合う2つの肺胞は、肺胞中隔内の1つの
毛細血管網を、その接する面で両方から共有する。 」(船戸和也のHP)


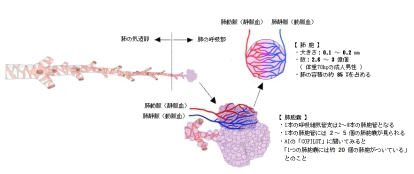

・1個の肺胞の表面積は約27万μ㎡で、一人当たり全体で70~80㎡の表面積となる。
「ウィキペディア」には以下のような解説文が見られる。
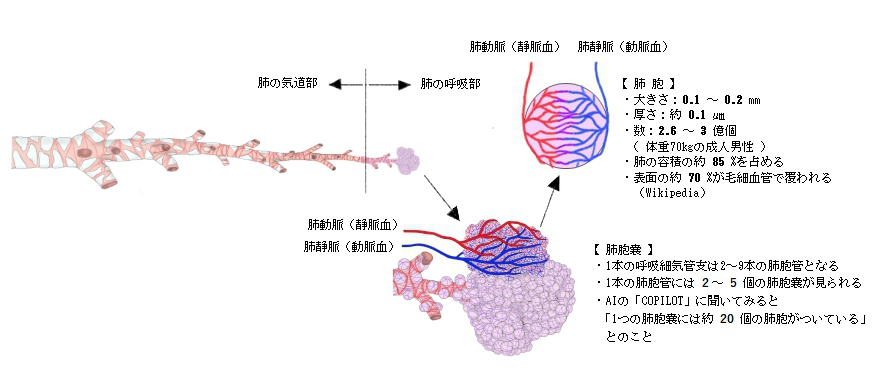
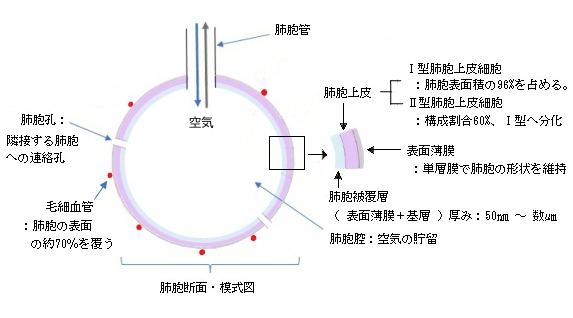
肺胞は、厚さ約0.1μmの扁平上皮である呼吸上皮細胞(肺胞上皮細胞)が
直径約0.1-0.2mmの球状になり、空洞(肺胞気)を取り囲む構造を持つ。
・The diameter of an alveolus is between 200 and 500 μm. (Wikipedia)


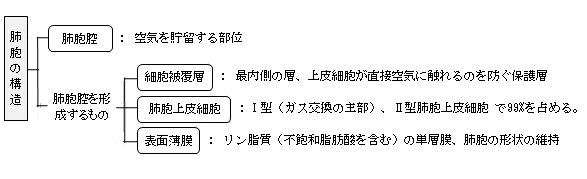
【構 造】
以下に「船戸和也のHP」を中心にして3種類の肺胞上皮細胞の特徴を記した。
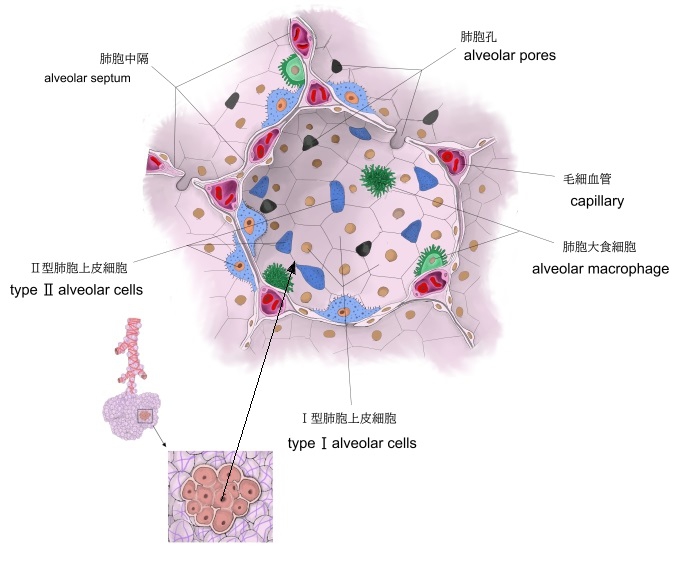
以下の3種類の細胞にプラスして肺胞には「肺胞大食細胞 alveolar macrophage
(または塵埃細胞 dust cell )」と呼ばれる貪食細胞が存在している。
⇒肺胞上皮細胞や関連する膜層の詳しい解説は「船戸和也のHP」を参照のこと
1 |
Ⅰ型肺胞上皮細胞
typeⅠ alveolar cell
|
・扁平肺胞上皮細胞とも
・構成割合:39% だが1個あたりの表面積が Ⅱ型の約36倍となる。従って

・非常に薄い扁平な細胞
細胞質の幅:100㎛(船戸和也のHP)
厚さ:AIに尋ねたところ「0.05~0.2㎛」との回答
ただし、「イメカラ」では「約0.0025㎛」としている。
・細胞同士は閉鎖帯で接着している。
|
2 |
Ⅱ型肺胞上皮細胞
typeⅡ alveolar cell
|
・構成割合:60% 下部の「注意」を参照のこと
・顆粒肺細胞、大肺胞細胞などとも。
・立方細胞で細胞頂に短い微絨毛を有する。
・界面活性剤を分泌⇒被膜層の主成分
・分裂機能を有しⅠ型に分化し得る。
|
3 |
Ⅲ型肺胞上皮細胞
typeⅢ alveolar cell
|
・構成割合:1%以下
・立方形で細胞頂に幅の太い微絨毛を有する。
・Ⅱ型細胞の傍らに位置することがほとんど。
|
【肺胞被覆層】 参考)船戸和也のHP
・肺胞被覆層は肺胞上皮細胞の内側に位置している。
・肺胞被覆層の存在によって肺胞上皮細胞は肺胞腔の空気に直接触れることはない。
・厚さは部位によって異なり50㎚から数㎛となる。
・Ⅱ型肺胞上皮細胞が層の形成に大きく関与しているが、一部Ⅰ型からも成分の供給を受ける。
・二層構造:表面薄膜(最内層)+基層
【表面薄膜】 参考)船戸和也のHP
・リン脂質(不飽和脂肪酸を含む)の単層膜
・肺胞の形状を維持
【関連語句】
以下は「Wikipedia」の解説文となる。
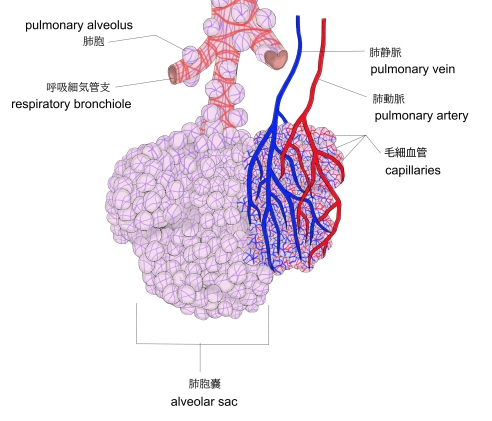
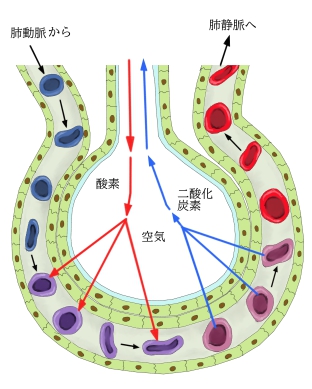
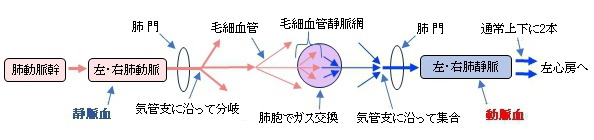
A pulmonary alveolus (pl.: alveoli, from Latin alveolus, "little cavity"), also known as an air sac or air space, is one of millions of hollow, distensible cup-shaped cavities in the lungs where pulmonary gas exchange takes place. Oxygen is exchanged for carbon dioxide at the blood–air barrier between the alveolar air and the pulmonary capillary.Alveoli make up the functional tissue of the mammalian lungs known as the lung parenchyma, which takes up 90 percent of the total lung volume.
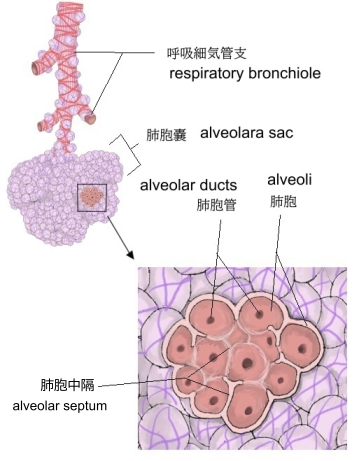
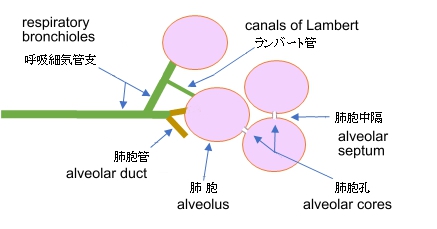
Alveoli are first located in the respiratory bronchioles that mark the beginning of the respiratory zone. They are located sparsely in these bronchioles, line the walls of the alveolar ducts, and are more numerous in the blind-ended alveolar sacs.The acini are the basic units of respiration, with gas exchange taking place in all the alveoli present. The alveolar membrane is the gas exchange surface, surrounded by a network of capillaries. Oxygen is diffused across the membrane into the capillaries and carbon dioxide is released from the capillaries into the alveoli to be breathed out.
Alveoli are particular to mammalian lungs. Different structures are involved in gas exchange in other vertebrates.
【Structure】
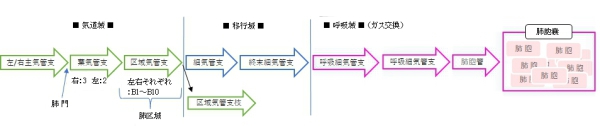
The alveoli are first located in the respiratory bronchioles as scattered outpockets, extending from their lumens. The respiratory bronchioles run for considerable lengths and become increasingly alveolated with side branches of alveolar ducts that become deeply lined with alveoli. The ducts number between two and eleven from each bronchiole. Each duct opens into five or six alveolar sacs into which clusters of alveoli open.
Each terminal respiratory unit is called an acinus and consists of the respiratory bronchioles, alveolar ducts, alveolar sacs, and alveoli. New alveoli continue to form until the age of eight years.
A typical pair of human lungs contains about 480 million alveoli, providing a total surface area for gas exchange of between 70 and 80 square metres. Each alveolus is wrapped in a fine mesh of capillaries covering about 70% of its area. The diameter of an alveolus is between 200 and 500 μm.
【語句】
・respiratory bronchioles: ・scattered: ・lumen:内腔? ・alveolar duct:肺胞管 ・alveolar sac:肺胞嚢 ・: ・: ・: ・: ・: ・: ・: ・: ・: ・: ・: ・: ・: ・: ・: ・: ・: ・: ・: ・: ・: ・: ・: ・: ・: ・: ・: ・: ・: ・: ・:
【Microanatomy】
An alveolus consists of an epithelial layer of simple squamous epithelium (very thin, flattened cells),[13] and an extracellular matrix surrounded by capillaries. The epithelial lining is part of the alveolar membrane, also known as the respiratory membrane, that allows the exchange of gases. The membrane has several layers – a layer of alveolar lining fluid that contains surfactant, the epithelial layer and its basement membrane; a thin interstitial space between the epithelial lining and the capillary membrane; a capillary basement membrane that often fuses with the alveolar basement membrane, and the capillary endothelial membrane. The whole membrane however is only between 0.2 μm at its thinnest part and 0.6 μm at its thickest.[14]
In the alveolar walls there are interconnecting air passages between the alveoli known as the pores of Kohn. The alveolar septum that separates the alveoli in the alveolar sac contains some collagen fibers and elastic fibers. The septa also house the enmeshed capillary network that surrounds each alveolus.[3] The elastic fibres allow the alveoli to stretch when they fill with air during inhalation. They then spring back during exhalation in order to expel the carbon dioxide-rich air.
There are three major types of alveolar cell. Two types are pneumocytes or pneumonocytes known as type I and type II cells found in the alveolar wall, and a large phagocytic cell known as an alveolar macrophage that moves about in the lumens of the alveoli, and in the connective tissue between them. Type I cells, also called type I pneumocytes, or type I alveolar cells, are squamous, thin and flat and form the structure of the alveoli. Type II cells, also called type II pneumocytes or type II alveolar cells, release pulmonary surfactant to lower surface tension, and can also differentiate to replace damaged type I cells.[12][15]
【Development】
Development of the earliest structures that will contain alveoli begins on day 22 and is divided into five stages: embryonic, pseudoglandular, canalicular, saccular, and alveolar stage.[16] The alveolar stage begins approximately 36 weeks into development. Immature alveoli appear as bulges from the sacculi which invade the primary septa. As the sacculi develop, the protrusions in the primary septa become larger; new septations are longer and thinner and are known as secondary septa.[16] Secondary septa are responsible for the final division of the sacculi into alveoli. Majority of alveolar division occurs within the first 6 months but continue to develop until 3 years of age. To create a thinner diffusion barrier, the double-layer capillary network fuse into one network, each one closely associated with two alveoli as they develop.[16]
In the first three years of life, the enlargement of lungs is a consequence of the increasing number of alveoli; after this point, both the number and size of alveoli increases until the development of lungs finishes at approximately 8 years of age.[16]
【Function】
Type I cells are the larger of the two cell types; they are thin, flat epithelial lining cells (membranous pneumocytes), that form the structure of the alveoli. They are squamous (giving more surface area to each cell) and have long cytoplasmic extensions that cover more than 95% of the alveolar surface.
Type I cells are involved in the process of gas exchange between the alveoli and blood. These cells are extremely thin – sometimes only 25 nm – the electron microscope was needed to prove that all alveoli are lined with epithelium. This thin lining enables a fast diffusion of gas exchange between the air in the alveoli and the blood in the surrounding capillaries.
The nucleus of a type I cell occupies a large area of free cytoplasm and its organelles are clustered around it reducing the thickness of the cell. This also keeps the thickness of the blood-air barrier reduced to a minimum.
The cytoplasm in the thin portion contains pinocytotic vesicles which may play a role in the removal of small particulate contaminants from the outer surface. In addition to desmosomes, all type I alveolar cells have occluding junctions that prevent the leakage of tissue fluid into the alveolar air space.
The relatively low solubility (and hence rate of diffusion) of oxygen necessitates the large internal surface area (about 80 square m [96 square yards]) and very thin walls of the alveoli. Weaving between the capillaries and helping to support them is an extracellular matrix, a meshlike fabric of elastic and collagenous fibres. The collagen fibres, being more rigid, give the wall firmness, while the elastic fibres permit expansion and contraction of the walls during breathing.
Type I pneumocytes are unable to replicate and are susceptible to toxic insults. In the event of damage, type II cells can proliferate and differentiate into type I cells to compensate.[18]
Type II cells[edit]
Type II cells are cuboidal and much smaller than type I cells.[3] They are the most numerous cells in the alveoli, yet do not cover as much surface area as the squamous type I cells.[18] Type II cells (granulous pneumocytes) in the alveolar wall contain secretory organelles known as lamellar bodies or lamellar granules, that fuse with the cell membranes and secrete pulmonary surfactant. This surfactant is a film of fatty substances, a group of phospholipids that reduce alveolar surface tension. The phospholipids are stored in the lamellar bodies. Without this coating, the alveoli would collapse. The surfactant is continuously released by exocytosis. Reinflation of the alveoli following exhalation is made easier by the surfactant, which reduces surface tension in the thin fluid lining of the alveoli. The fluid coating is produced by the body in order to facilitate the transfer of gases between blood and alveolar air, and the type II cells are typically found at the blood–air barrier.[19][20]
Type II cells start to develop at about 26 weeks of gestation, secreting small amounts of surfactant. However, adequate amounts of surfactant are not secreted until about 35 weeks of gestation – this is the main reason for increased rates of infant respiratory distress syndrome, which drastically reduces at ages above 35 weeks gestation.
Type II cells are also capable of cellular division, giving rise to more type I and II alveolar cells when the lung tissue is damaged.[21]
MUC1, a human gene associated with type II pneumocytes, has been identified as a marker in lung cancer.[22]
The importance of the type 2 lung alveolar cells in the development of severe respiratory symptoms of COVID-19 and potential mechanisms on how these cells are protected by the SSRIs fluvoxamine and fluoxetine was summarized in a review in April 2022.[23]
Alveolar macrophages[edit]
The alveolar macrophages reside on the internal luminal surfaces of the alveoli, the alveolar ducts, and the bronchioles. They are mobile scavengers that serve to engulf foreign particles in the lungs, such as dust, bacteria, carbon particles, and blood cells from injuries.[24] They are also called pulmonary macrophages, and dust cells.
【語句】
・: ・: ・: ・: ・: ・: ・: ・: ・: ・: ・: ・: ・: ・: ・: ・: ・: ・: ・: ・: ・: ・: ・: ・: ・: ・: ・: ・: ・: ・: ・: ・: ・: ・: ・: ・:
■ 写真やイラストを掲載しているサイト ■
・ イラストや写真を掲載しているサイト-Ⅰ
・ イラストや写真を掲載しているサイト-Ⅱ
・ イラストや写真を掲載しているサイト-Ⅲ
・ イラストや写真を掲載しているサイト-Ⅳ
・ イラストや写真を掲載しているサイト-Ⅴ
|